
INTRODUCTION — Since Reginald Fitz presented the first comprehensive description of appendicitis and advocated early surgical removal of the appendix in 1886, appendicitis has been recognized as one of the most common causes of the acute abdomen worldwide. Acute appendicitis is one of the most frequent indications for abdominal surgery.
Appendicitis occurs most frequently in the second and third decades of life. The incidence is highest in the 10- to 19-year-old age group, in which it is about 233/100,000 population. It is also higher among men (male to female ratio of 1.4:1) who have a lifetime incidence of 8.6 percent compared to 6.7 percent for women .
The goal of therapy is early diagnosis and prompt operative intervention. However, the diagnosis of appendicitis can be difficult, especially in patients less than 3 years of age, pregnant, and older than age 60 years . In the younger and older age groups the diagnosis is often delayed, leading to perforation rates as high as 80 percent . The diagnosis can be challenging in pregnant women, especially in the second and third trimesters, due to the displacement of the appendix by the uterus and the resulting changes in the physical examination.
The clinical manifestations and diagnosis of appendicitis in adults will be reviewed here. The management of appendicitis, appendicitis in pregnancy, and the diagnosis and differential diagnosis of abdominal pain in adults are discussed separately.
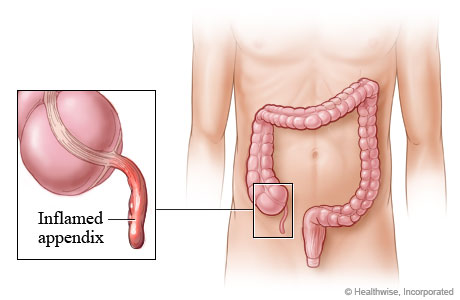
ANATOMY — The veriform appendix is located near the ileocecal valve where the taenia coli converge on the cecum . The appendix is considered a true diverticulum of the cecum. In contrast to acquired diverticular disease, which consists of a protuberance of a subset of the enteric wall layers, the appendiceal wall contains all of the layers of the colonic wall: mucosa, submucosa, muscularis (longitudinal and circular), and the serosal covering .
The appendiceal orifice opens into the cecum. The appendix is located at the base of the cecum at the confluence of the three taenia coli. Its blood supply, the appendiceal artery, is a terminal branch of the ileocolic artery, which traverses the length of the mesoappendix and terminates at the tip of the organ .
The attachment of the appendix to the base of the cecum is constant. However the tip may migrate to the retrocecal, subcecal, preileal, postileal and pelvic positions. These normal anatomic variations can complicate the diagnosis as the site of pain and findings on the clinical examination will reflect the anatomic position of the appendix.
The presence of B and T lymphoid cells in the mucosa and submucosa of the lamina propria make the appendix histologically distinct from the nearby cecum . These cells create a lymphoid pulp that aid immunologic function by increasing lymphoid products such as IgA and operating as part of the gut-associated lymphoid tissue system . Lymphoid hyperplasia can cause obstruction of the appendix and lead to appendicitis. The lymphoid tissue undergoes atrophy with age, which may account for the age distribution seen in acute appendicitis .
PATHOGENESIS — The natural history of appendicitis is similar to that of other inflammatory processes involving hollow visceral organs. Initial inflammation of the appendiceal wall is followed by localized ischemia, perforation, and the development of a contained abscess or generalized peritonitis.
Appendiceal obstruction has been proposed as the primary cause of appendicitis . Obstruction is frequently implicated but not always required for the development of appendicitis. A study of patients with appendicitis showed that there was elevated intraluminal pressure in only one third of the patients with nonperforated appendicitis .
Appendiceal obstruction may be caused by fecaliths (hard fecal masses), calculi, lymphoid hyperplasia, infectious processes, and benign or malignant tumors. However, some patients with a fecalith have a histologically normal appendix and the majority of patients with appendicitis do not have a fecalith .
When obstruction of the appendix is the cause of appendicitis, the obstruction leads to an increase in luminal and intramural pressure, resulting in thrombosis and occlusion of the small vessels in the appendiceal wall, and stasis of lymphatic flow. As the appendix becomes engorged, the visceral afferent nerve fibers entering the spinal cord at T8-T10 are stimulated, leading to vague central or periumbilical abdominal pain . Well-localized pain occurs later in the course when inflammation involves the adjacent parietal peritoneum.
The mechanism of luminal obstruction varies depending upon the patient's age. In the young, lymphoid follicular hyperplasia due to infection is thought to be the main cause. In older patients, luminal obstruction is more likely to be caused by fibrosis, fecaliths, or neoplasia (carcinoid, adenocarcinoma, or mucocele). In endemic areas, parasites can cause obstruction in any age group. (See "Cancer of the appendix and pseudomyxoma peritonei".)
Once obstructed, the lumen becomes filled with mucus and distends, increasing luminal and intramural pressure. This results in thrombosis and occlusion of the small vessels, and stasis of lymphatic flow. As lymphatic and vascular compromise progress, the wall of the appendix becomes ischemic and then necrotic.
Bacterial overgrowth occurs within the diseased appendix. Aerobic organisms predominate early in the course, while mixed infection is more common in late appendicitis. Common organisms involved in gangrenous and perforated appendicitis include Escherichia coli, Peptostreptococcus, Bacteroides fragilis, and Pseudomonas species . Intraluminal bacteria subsequently invade the appendiceal wall and further propagate a neutrophilic exudate. The influx of neutrophils causes a fibropurulent reaction on the serosal surface, irritating the surrounding parietal peritoneum . This results in stimulation of somatic nerves, causing pain at the site of peritoneal irritation .
A model that separates the pathogenesis of nonperforating from perforating appendicitis has been proposed . It is thought that the type of luminal obstruction may be a predictor of appendicitis leading to perforation. Further reinforcement of this theory came from research into the types of fecaliths and calculi that can be found in the appendix. Fecaliths were six times more common than true calculi, but calculi were more often associated with perforated appendicitis or periappendiceal abscess (45 per cent) than were fecaliths (19 per cent). This is presumably due to the rigidity of true calculi as compared to the softer, more crushable fecaliths .
Once significant inflammation and necrosis occur, the appendix perforates, leading to localized abscess formation or diffuse peritonitis. During the first 24 hours after symptoms develop, approximately 90 percent of patients have inflammation and perhaps necrosis of the appendix, but not perforation.
The time course to perforation is variable. One study showed that 20 percent of patients developed perforation less than 24 hours after the onset of symptoms . Sixty-five percent of patients in whom the appendix perforated had symptoms for longer than 48 hours.
A perforated appendix must be considered in a patient whose temperature exceeds 103.0ºF (39.4ºCelsius). The same considerations apply for an elevated white blood cell count. Many patients will have a mild leukocytosis of up to 15 X 10(3)/mm(3). Perforation is more likely to have occurred in patients with a higher leukocyte count.
CLINICAL MANIFESTATIONS — Abdominal pain is the most common clinical symptom of appendicitis, and is found in nearly all confirmed cases . The clinical presentation of acute appendicitis is described as a constellation of "classic" signs and symptoms:
• Right lower quadrant (right iliac fossa) abdominal pain
• Anorexia
• Nausea and vomiting
In the "classic" presentation, the patient describes the onset of abdominal pain as the first symptom. The pain is periumbilical in nature with subsequent migration to the right lower quadrant as the inflammation progresses . Nausea and vomiting, if they occur, usually follow the onset of pain. Fever and leukocytosis follow later in the course of illness. Low grade fever up to 101.0ºF (38.3ºC) may be present.
Nevertheless, in many patients, initial features are atypical or nonspecific, and can include:
• Indigestion
• Flatulence
• Bowel irregularity
• Diarrhea
• Generalized malaise
Because the early signs and symptoms of appendicitis are often subtle, patients and clinicians may downplay their importance. Although considered a classic symptom, migratory pain that begins in the periumbilical region and then moves to the right lower quadrant occurs only in 50 to 60 percent of patients with appendicitis .
The symptoms of appendicitis can vary depending upon the location of the appendix. An inflamed anterior appendix produces marked symptoms in the right lower quadrant, while a retrocecal appendix may not cause the same degree of local signs of peritonitis because the inflammation is masked by the overlying bowel.
No single feature or combination of features is a highly accurate predictor of acute appendicitis, although prediction rules based upon combinations of features may have some clinical utility .
DIFFERENTIAL DIAGNOSIS — A variety of inflammatory conditions in the right lower quadrant can mimic appendicitis.
Cecal diverticulitis — Cecal diverticulitis usually occurs in young adults and presents with signs and symptoms that are virtually identical to those of appendicitis.
Meckel's diverticulitis — Meckel's diverticulitis presents in a fashion similar to appendicitis. A Meckel's diverticulum is a congenital remnant of the omphalomesenteric duct. It contains all layers of the intestine and may have ectopic tissue present from either the pancreas or stomach. It is located on the small intestine two feet from the ileocecal valve, and is about two inches in length .
Meckel's diverticulitis should be included in the differential diagnosis as the small bowel may migrate into the right lower quadrant and mimic the symptoms of appendicitis. Other complications associated with a Meckel's diverticulum include bleeding if it contains ectopic gastric mucosa, and an obstruction due to the diverticulum serving as a leading edge for an intussusception or an internal hernia. If an inflamed appendix is not found on abdominal exploration for acute appendicitis, the surgeon should search for an inflamed Meckel's diverticulum.
Acute ileitis — Acute ileitis due most commonly to an acute self-limited bacterial infection (Yersinia, Campylobacter, Salmonella, and others), should be considered when diarrhea is a prominent symptom.
Crohn's disease — Crohn's disease can present with symptoms similar to appendicitis. Fatigue, prolonged diarrhea with abdominal pain, weight loss, and fever, with or without gross bleeding are the hallmarks of Crohn's disease. Crohn's disease should be suspected in patients who have persistent pain after surgery, especially if the appendix is histologically normal.
Gynecologic conditions — A number of gynecologic conditions, most notably ectopic pregnancy and pelvic inflammatory disease (acute salpingitis), should be considered in the differential diagnosis.
PHYSICAL EXAMINATION — The patient should undergo a careful physical examination, including a rectal examination. Women should undergo a pelvic examination.
The physical examination may be unrevealing in the very early stages of appendicitis since the visceral organs are not innervated with somatic pain fibers. However, as the inflammation progresses, involvement of the overlying parietal peritoneum causes localized tenderness in the right lower quadrant. This may be detected with abdominal examination, or during rectal and pelvic examination.
Patients with a retrocecal appendix are an exception since the appendix does not come into contact with the anterior parietal peritoneum. In such patients, localized tenderness may be less impressive. These patients often complain of a dull ache instead of the localized tenderness that is seen with an inflamed appendix in the anterior iliac fossa. Rectal or pelvic examination in such patients is more likely to elicit symptoms than abdominal examination.
The location of the pain may also be atypical in patients who have a pelvic appendix, which can cause tenderness below McBurney's point. Such patients often complain of urinary frequency and dysuria or rectal symptoms, such as tenesmus and diarrhea.
Several findings on physical examination have been described to facilitate diagnosis:
• McBurney's point tenderness is described as maximal tenderness at 1.5 to 2 inches from the anterior superior iliac spine (ASIS) on a straight line from the ASIS to the umbilicus. (Sensitivity 50 to 94 percent; specificity 75 to 86 percent ).
• Rovsing's sign refers to pain in the right lower quadrant with palpation of the left lower quadrant. This sign is also called indirect tenderness and is indicative of right-sided local peritoneal irritation . (Sensitivity 22 to 68 percent; specificity 58 to 96 percent ).
• The psoas sign is indicative of a retrocecal appendix. This is manifested by right lower quadrant pain with right hip flexion. The inflamed appendix may lie against the right psoas muscle, causing the patient to shorten the muscle by drawing up the right knee. Passive extension of the iliopsoas muscle with hip extension causes right lower quadrant pain. (Sensitivity 13 to 42 percent; specificity 79 to 97 percent ).
• The obturator sign is indicative of a pelvic appendix. This test is based on the principle that the inflamed appendix may lie again the right obturator internus muscle. When the clinician flexes the patient's right hip and knee followed by internal rotation of the right hip, this elicits right lower quadrant pain. (Sensitivity 8 percent; specificity 94 percent ).
LABORATORY STUDIES — Laboratory tests serve a supportive role in the diagnosis of appendicitis as the diagnosis is made primarily on clinical findings. No single laboratory test or combination of tests is an absolute marker for appendicitis . Howwever, laboratory tests are useful and patients with an acute abdomen should have a complete blood count (CBC) with a differential to identify a leukocytosis. Approximately 80 percent of patients with appendicitis have a preoperative leukocytosis (white cells >10,000 cells/uL) and a left shift in the differential . It is important to remember that a leukocytosis can be present in other acute etiologies of abdominal pain. However, acute appendicitis is unlikely when the WBC is normal . In addition, a pregnancy test should be performed for all women of childbearing age.
Interestingly, mild elevations in serum bilirubin (total bilirubin >1.0 mg/dL) have been noted to be a marker for appendiceal perforation with a sensitivity of 70 percent and a specificity of 86 percent. This compares favorably with a sensitivity and specificity of an elevated WBC of 80 percent and 55 percent respectively.
CLINICAL ASSESSMENT — The constellation of findings from history, physical examination, and laboratory studies can often lead an experienced examiner to the correct diagnosis of appendicitis without further imaging . Several studies have found the diagnostic accuracy of clinical evaluation alone to be 75 to 90 percent . The diagnostic accuracy of the clinical examination may depend on the experience of the examining clinician .
Patients in whom appendicitis is considered to be extremely likely after assessment by an experienced clinician should proceed to appendectomy without further radiologic testing.
Diagnostic scoring systems — Several scoring systems have been proposed to standardize the correlation of clinical and laboratory variables. The Alvarado score is the most widely used diagnostic aid for the diagnosis of appendicitis and has been modified slightly since it was introduced.
The modified Alvarado scale assigns a score to each of the following diagnostic criteria:
• Migratory right iliac fossa pain (1 point)
• Anorexia (1 point)
• Nausea/vomiting (1 point)
• Tenderness in the right iliac fossa (2 points)
• Rebound tenderness in the right iliac fossa (1 point)
• Fever >37.5 degrees C (1 point)
• Leukocytosis (2 points)
The points totals are used to guide management:
• A patient with a score of 0 to 3 could be considered to have a low risk of appendicitis and would be discharged with advice to return if there was no improvement in symptoms, subject to social circumstances.
• A patient with a score of 4 to 6 would be admitted for observation and re-examination. If the score remains the same after 12 hours, operative intervention is recommended.
• A male patient with a score of 7 to 9 would proceed to appendectomy.
• A female patient who is not pregnant would undergo diagnostic laparoscopy, then appendectomy if indicated by the intraoperative findings. The surgical management of appendicitis in pregnancy is discussed separately.
In validation studies, the Alvarado score had a sensitivity of 95 percent for appendicitis with a score greater than 7 and overall accuracy of 83 percent . However, it is more accurate in men and children than in women .
Accuracy of the score appears to be lower in women . Some have advocated diagnostic laparoscopy to minimize the high false-negative rate in women . Others have suggested using CT scans to help with the diagnosis of patients with equivocal clinical presentation and a score of 4 to 6.
Several other scoring systems have been described as well . A systematic review of several published scoring systems showed a diagnostic sensitivity of 53 to 99 percent and specificity of 30 to 99 percent . As a general rule, the addition of these decision aids to clinical judgment has the potential to improve specificity and lead to lower false-positive rates in diagnosis of acute appendicitis, but decision aids cannot definitively determine or exclude the possibility of appendicitis .
RADIOGRAPHIC STUDIES — Over the last few decades, there has been increasing use of imaging modalities such as ultrasonography (US) and computed tomography (CT) in the diagnosis of acute appendicitis. Although the increased use of imaging has decreased the rate of negative appendectomies , many surgeons will proceed with surgical exploration, in the absence of imaging, if there is a strong clinical concern for appendicitis.
The acceptable number of negative appendectomies varies depending upon the age and sex of the patient. For example, in young healthy males with right lower quadrant pain, the negative appendectomy rate (NAR) should be less than 10 percent, while a rate that approaches 20 percent is reasonable in young women in whom other pelvic processes can make accurate diagnosis more difficult . A low NAR has been achieved in some centers that use close in-hospital observation .
Although diagnostic imaging is unnecessary when the diagnosis of appendicitis is certain, imaging should be performed when the diagnosis of appendicitis is suspected but unclear. Diagnostic imaging is especially useful in several subpopulations, including children, elder adults, or women of childbearing age. Similarly, patients with comorbidities such as diabetes, obesity, and immunocompromise may have a higher occurrence of atypical presentation of appendicitis. These populations are more likely to present with unclear symptoms such as vague abdominal pain.
Women of childbearing age, as well as elder adults, have a higher rate of negative appendectomy. Several studies have demonstrated that women were more than twice as likely as men to undergo a negative appendectomy and therefore benefit from standardized imaging in the evaluation of suspected appendicitis . A study of 1425 consecutive patients undergoing appendectomy over a seven-year period at a single institution found that preoperative CT scanning was particularly useful in women and contributed to a significant reduction in NAR (from 21 to 8 percent) .
Imaging is also useful for elder adults and patients with significant comorbidities, in whom the clinical findings may be atypical for appendicitis.
Computed tomography (CT) — Many studies have evaluated the diagnostic accuracy of CT scan for appendicitis in comparison to clinical examination. Patients with suspected appendicitis can often be categorized into those with clinical findings that are highly predictive of the presence or absence of appendicitis and those with an equivocal clinical picture. Some studies comparing evaluation by surgical attendings with findings of CT scan have found statistically similar diagnostic accuracy in the assessment of patients presenting with an equivocal examination . Other studies have found that CT findings influence the treatment plan; in one such report, the CT scan changed the treatment plan for 58 percent of patients . Differences in studies may in part be due to the experience of the clinical assessor and the populations being studied.
Several CT protocols for imaging the appendix have been described, three protocols are mainly used. These include:
• Standard abdominal-pelvic CT with IV and oral contrast
• Focused appendiceal CT with rectal contrast
• Non-contrast CT
In most cases, if there is enough diagnostic concern and uncertainty to warrant a CT scan for appendicitis, a full abdominal-pelvic CT with IV and oral contrast should be performed or a decision should be made to proceed to the operating room for abdominal exploration.
Standard CT with contrast — A commonly used protocol involves a standard abdominal and pelvic CT scan (16-MDCT or higher) with intravenous and oral contrast.
A number of findings suggest acute appendicitis on standard abdominal CT scanning :
• Enlarged appendiceal diameter >6 mm with an occluded lumen
• Appendiceal wall thickening (>2 mm)
• Periappendiceal fat stranding
• Appendiceal wall enhancement
• Appendicolith
The sensitivity and specificity of CT with IV and oral contrast for acute appendicitis is in the range of 91 to 98 and 75 to 93 percent, respectively . Air in the appendix or a contrast filled lumen in a normal appearing appendix virtually excludes the diagnosis. However, a nonvisualized appendix does not rule out appendicitis. This is particularly important to remember in patients who have had symptoms for a short duration, since only minimal inflammatory changes may be present in the right lower quadrant.
An advantage of a complete abdominal CT scan is that it permits visualization of the entire abdomen. An alternative diagnosis is found in up to 15 percent of patients . Furthermore, a CT scan can assist in the treatment plan for patients with a palpable abdominal mass, such as those in whom an appendiceal phlegmon or abscess may have developed. These features are more likely in patients who present after having prolonged symptoms (four to five days).
A drawback of the standard CT protocol is that it takes up to two hours to administer oral contrast. In addition a CT scan involves radiation exposure and intravenous contrast, with the potential for contrast-induced renal nephropathy. Cost and availability are also considerations, particularly in resource-poor settings.
Appendiceal CT — A focused appendiceal CT scan can be performed with rectal contrast alone and thin cuts through the right iliac fossa. Because full oral contrast is not given, the scan can be performed within 15 minutes. Rectal contrast provides good visualization of the pericecal region without the need to wait for oral contrast to reach the right lower quadrant.
In a report using a limited appendiceal CT scan with rectal contrast, the sensitivity of the most common findings for acute appendicitis were as follows :
• Right lower abdominal quadrant fat stranding (100 percent sensitivity)
• Focal cecal thickening (69 percent specificity)
• Adenopathy (63 percent sensitivity)
One study reported that a focal appendiceal CT had 98 percent accuracy and sensitivity with rectal contrast along a limited area (15 cm) of the pelvis centered 3 cm superior to the cecal tip.
The relevance of focal appendiceal imaging is questionable outside of large medical centers, as this technique requires personnel to administer rectal contrast and a radiologist on site for the verification of positioning. In addition, an appendiceal CT scan only looks at the appendix, and the images may be unrevealing in the presence of other abdominal pathology. As a result, evaluation should continue in patients with a negative study.
Unenhanced CT — The administration of contrast for imaging adds time, expense, and risk of an allergic reaction to the contrast agent. A number of studies have suggested that adequate imaging can be obtained without contrast. In various reports, unenhanced CT had a sensitivity of 88 to 96 percent, specificity of 91 to 98 percent, and diagnostic accuracy of 94 to 97 percent for appendicitis, with the added advantage of total exam time of 5 to 15 minutes.
Test characteristics may depend at least in part upon the patient's body habitus . Some radiologists maintain that if the BMI exceeds 25 that the CT is less accurate and therefore oral contrast is necessary.
An important limitation of unenhanced CT is the limited ability to diagnose other abdominal pathology, potentially diminishing the role of the examination in patients in whom there is diagnostic uncertainty (ie, those in whom imaging may be most important).
Unenhanced CT may be of some value in patients who have renal failure or clinical instability. However, for most patients where there is sufficient diagnostic uncertainty to warrant a CT scan for appendicitis, a full abdominal-pelvic CT with IV and oral contrast should be performed or a decision should be made to proceed to the operating room for abdominal exploration.
Ultrasonography — Ultrasound (US) is generally considered to be reliable for ruling-in acute appendicitis, but cannot be trusted to rule it out. It has little added value when the clinical presentation is clear.
At least eight sonographic internal inflammatory changes of the appendix have been described [11,43,88]. The most accurate ultrasound finding for acute appendicitis is an appendiceal diameter of >6 mm with a sensitivity, specificity, negative predictive value and positive predictive value of 98 percent. In various reports, the sensitivity and specificity by US in the diagnosis of appendicitis ranged from 35 to 98 percent and 71 to 98 percent, respectively .
Advantages compared with CT include the ability to obtain results quickly, and lack of radiation exposure or need for contrast agents. An added benefit is that it can also be useful for defining pelvic pathology in women. Endovaginal ultrasound is particularly sensitive for evaluating the female reproductive tract. The roles of ultrasonography in evaluation of appendicitis during pregnancy and in children are described separately.
The disadvantages of ultrasonography are that it is not as accurate as CT for diagnosis of appendicitis and is less likely to reveal alternative diagnoses. Furthermore, accuracy is operator dependent and it may be difficult to image patients with a large body habitus or those who have a large amount of overlying bowel gas. As a general rule, the main role of ultrasonography is to help confirm the diagnosis of suspected appendicitis, particularly in women.
Plain radiographs — Plain radiographs are usually not helpful for establishing the diagnosis of appendicitis. However, the following radiographic findings have been associated with acute appendicitis:
• Right lower quadrant appendicolith
• Localized right lower quadrant ileus
• Loss of the psoas shadow
• Free air (occasionally)
• Deformity of cecal outline
• Right lower quadrant soft tissue density
Imaging costs — The increase in the use of CT scanning for the diagnosis of appendicitis has been largely justified by the assumption that it decreases the rates of perforated appendicitis as well as nontherapeutic appendectomies . In two studies that performed cost analysis, one showed that the cost of nontherapeutic appendectomy was 16 times more expensive than a focused appendiceal CT scan, while another reported that appendectomy was 22 times more expensive than non-enhanced CT scanning, implying cost savings if a reduction in nontherapeutic appendectomy rates could be achieved .
Several studies have failed to demonstrate a significant reduction in the overall institutional rates for nontherapeutic appendectomies despite the increased use of CT scan over time. Results of studies that included analysis of perforated appendicitis are mixed. One study showed an observed rate of appendiceal perforation of 9 percent in patients who underwent routine CT imaging compared to 25 percent in patients in whom CT scanning was not used . Other studies have demonstrated a fairly constant rate of perforated appendix over time despite the increased use of CT scan.
Cost analysis for studies such as these is complicated by the value of CT scanning in patients in whom therapeutic appendectomy was performed; as a result, the cost savings depends upon an absolute rate reduction for nontherapeutic appendectomies . Additionally, cost calculations depend upon local institutional variables and surgeon variables; selected institutional observations may not be applicable to all practices.
SUMMARY AND RECOMMENDATIONS
• Acute appendicitis is one of the most common causes of an acute abdomen. The goal of therapy is early diagnosis and prompt operative intervention.
• The position of the appendix can vary significantly between individuals. The appendix can be found in a retrocecal or pelvic location, as well as medial, lateral, anterior or posterior to the cecum. Anatomic variability can complicate the diagnosis as clinical presentation will reflect the anatomic position of the appendix.
• Appendiceal obstruction plays a role in the pathogenesis of appendicitis, but it is not required for the development of appendicitis.
• The "classic" symptoms of appendicitis include right lower quadrant abdominal pain, anorexia, fever, nausea and vomiting. The abdominal pain is initially periumbilical in nature with subsequent migration to the right lower quadrant as the inflammation progresses.
• Not all patients will appendicitis will have the "classic" symptoms. Many patients with appendicitis present with atypical or nonspecific symptoms, such as indigestion, flatulence, bowel irregularity, and generalized malaise. Not all patients will have migratory pain and symptoms can vary depending upon the location of the appendix, especially when the appendix is retrocecal or pelvic. (See 'Clinical manifestations' above.)
• The constellation of findings from history, physical examination, and laboratory studies will usually lead an experienced examiner to the correct diagnosis of appendicitis without further imaging. Diagnostic scoring systems can be helpful in the diagnosis of acute appendicitis but cannot definitively rule out the possibility of appendicitis.
• Patients in whom appendicitis is considered to be extremely likely after assessment by an experienced clinician should proceed to appendectomy without further radiologic testing. A diagnostic laparoscopy should be considered for women of child-bearing age as this can help minimize the negative appendectomy rate.
• Diagnostic imaging should be performed when the diagnosis of appendicitis is suspected but unclear. We suggest a standard abdominal CT scan with intravenous and oral or rectal contrast.
• A variety of inflammatory conditions in the right lower quadrant can mimic appendicitis and should be considered in differential diagnosis.
 Subscribe to email feed
Subscribe to email feed



